Chemosis
Definition
Chemosis of the eye is a medical condition, in which the conjunctiva of the eye becomes swollen. The condition mainly caused by the exudation of the small capillaries of the eye, presenting an abnormal permeability. Chemosis occurs when the eye has been irritated, representing however a nonspecific sign. Upon a closer look, the conjunctiva will appear as if having liquid in it. The inflammation of the conjunctiva leads to an overall gelatinous appearance. The degree of the swelling varies from one patient to the other and, sometimes, it can become so inflamed, that the patient will have difficulties closing the eye (completely or partially). Due to the inflammation, the eyeball might appear as if moved from its original position (it should also be noted that the eyeball is not covered by the excess fluid).
Symptoms of Chemosis
These are the most common symptoms of chemosis:
- Inflammation of the conjunctiva
- The eyes appear to be red and watery
- Excessive tearing can occur because of the inflammation
- Itchiness is also present in some patients (often aggravated by the excessive rubbing of the eyes, predisposing to secondary bacterial infections)
- The vision can be affected by the inflammation of the conjunctiva (blurry or double)
- Gelatinous appearance of the conjunctiva
- The eyeball appear to have moved from its original position, due to the inflammation
- The patient might not be able to close his/her eye, due to the inflammation (the eyelids can become inflamed as well)
If you are experiencing intense pain in the eye or severe inflammation, you might be experiencing a severe allergic reaction. Keep in mind that severe allergic reactions are often accompanied by systemic symptoms, such as the increased heart rate, the wheezing and the swelling of the throat tissues, causing difficulties breathing. Emergency treatment is necessary before the symptoms of the allergic reaction become life-threatening.
Causes
These are the most common causes that lead to the appearance of chemosis:
- Allergy – seasonal allergies can lead to chemosis, as well as to itchiness and watery eyes
- Viral infection – there are different viruses that can lead to the inflammation of the conjunctiva (often transmitted through objects of personal hygiene, such as towels)
- Obstruction of the superior vena cava (the diagnosis can be confirmed if the patient presents facial edema as well)
- Thyroid disorders – the chemosis is present in people who have been diagnosed with hyperthyroidism (the other symptoms of the condition include the bulging of the eyes, the puffiness that surrounds the orbits of the eyes, the retraction or lag of the lids)
- Thrombosis of the cavernous sinus – this is a serious condition, in which a blood clot forms at the level of the cavernous sinus, which is actually a cavity at the base of the brain (drains blood from the brain, sending it to the heart). This condition is often associated with the infection of the paranasal sinuses, leading to a wide range of other symptoms, besides the chemosis: sensory loss at the level of the trigeminal nerve, abnormal movements at extraocular level, hemorrhage at the level of the retina, papilledema, edema around the orbits and bulging of the eyes.
- Carotid-cavernous fistula – this condition has a classic triad of symptoms, including the ocular bruit and the pulsatile bulging of the eyes, besides the actual chemosis
- Cluster headaches – neurological disorder, in which the patient suffers from recurrent headaches, most commonly unilateral and around the eye
- Trichinellosis – parasitic disease, caused by eating infected, raw or undercooked meat (pork/wild game)
- Systemic lupus erythematosus – autoimmune disease of the connective tissue, in which the immune system attacks the healthy tissues of the body
- Angioedema – severe allergic reaction, which can lead to suffocation if emergency treatment is not administered
- Acute glaucoma – increased pressure inside the eye (considered a medical emergency as well)
- Panophthalmitis – inflammation of the eye coats, including at the intraocular level
- Orbital cellulitis – severe inflammation of the eye tissues, often caused by an acute infection that has spread into the eye socket
- Gonorrheal conjunctivitis – infection transmitted through sexual intercourse, may cause extensive damage at the level of the eye, if proper treatment is not administered
- Dacryocystitis – infection of the lacrimal sac, which appears due to the obstruction of the nasolacrimal duct
- Urticaria – dermatologic disorder, often appears as an allergic reaction after the exposure to different allergens
- Rhabdomyosarcoma of the orbit – rare, malignant tumor, presenting a high risk of death.
Diagnosis
The diagnosis of chemosis is made through the following methods:
- Patient anamnesis – the doctor will ask a series of questions, such as:
- When did you notice the changes in your eyes?
- Do you present other symptoms, such as itchiness or excess watering?
- Do you know yourself to be allergic to any substances?
- Physical examination – using specific ophthalmologic instruments, the doctor will take a closer look at the eye
- Biopsy – this is recommended only when there is a suspicion of a tumor
Treatment
In order for the symptoms of chemosis to improve, one must first treat the underlying condition. Symptomatic treatment can also be administered, guaranteeing an improvement in the symptoms experienced by the patient.
These are the most common treatments recommended for chemosis:
Anti-histamines
- These are recommended in patients who suffer from allergies, reducing the inflammation of the conjunctiva and bringing relief from the other symptoms experienced (pain, itchiness)
- May be recommended as oral or topical administration (depending on the severity of the inflammation and the presence of other symptoms)
Antibiotics
- These are recommended in case of secondary bacterial infections, which may appear due to the excessive rubbing of the eyes
- The antibiotics should be taken for as long as they are prescribed, otherwise the bacteria will develop resistance to the treatment
- Probiotics are administered for the duration of the treatment, so as to maintain a healthy intestinal flora
Anti-inflammatory medication
- Topical or oral administration
- Reduce the inflammation and bring the necessary relief from the other symptoms (pain, itchiness)
Adrenaline
- Administered as emergency treatment, in case of severe allergic reactions
- Patients who know that they are allergic usually carry these allergy shots (immediate intervention is necessary, before the symptoms become life-threatening)
When to see a doctor
If you have noticed that the conjunctiva of your eyes has swollen all of a sudden, you must visit the doctor and ask for a consultation. At the same time, it is important to not delay going to the doctor, as you might be experiencing an allergic reaction. The doctor will perform a series of tests, in order to determine the things you are allergic to. If you are having difficulties breathing and you feel like you are suffocating, you are most likely experiencing a severe allergic reaction. In this situation, you have to call 911 and request immediate medical intervention. If the doctor discover that you are allergic to certain products, you will have to avoid them in the future and carry an allergy shot, just in case of emergency.
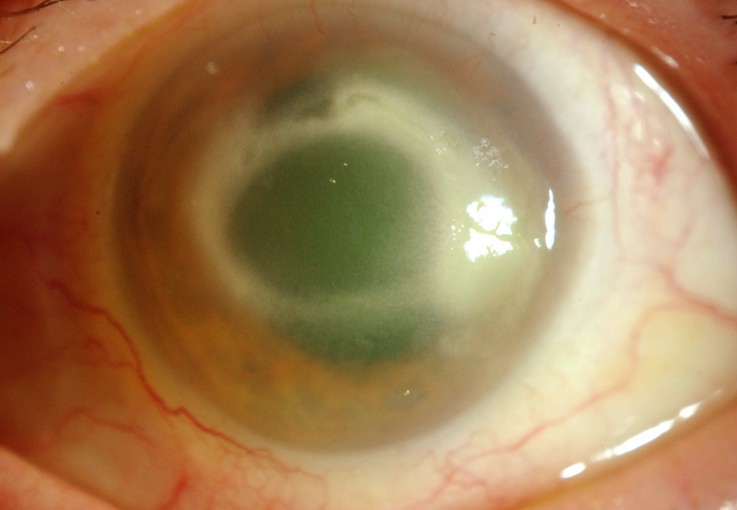
Chemosis Pictures
Here is how chemosis of the eye looks like…