Sialolithiasis
Sialolithiasis is a medical condition, in which calculi or stones form within the salivary glands. The most common appearance is at the level of the submandibular gland, this being also known as Wharton’s duct. It is also possible (however, it only occurs rarely) that the calculi appear at the level of the smaller salivary glands, as well as in the sublingual or parotid gland.
As you will have the opportunity to read below, two of the most important symptoms of this condition are inflammation and pain at the level of the respective salivary gland. The symptoms are usually aggravated by the stimulation of the salivary gland (seeing, thinking, smelling or tasting food), as well as by the mechanical actions in the area (chewing the food). Because of the association with food, sialolithiasis is often presented as the mealtime syndrome. There are different causes that can lead to the appearance of sialolithiasis, including chronic infections of the salivary glands, dehydration and autoimmune conditions (Sjögren’s syndrome). There are a lot of patients in which no exact cause can be identified.
The treatment, as you will see, requires the removal of the calculi through specific techniques. In the situation that the patient suffers from recurrent salivary stones, the surgeon might decide to remove the submandibular gland completely. This condition is quite common, affecting adults in general. Sialolithiasis is also more prevalent in the male population.
The salivary stones have different shapes and sizes; their texture and consistency vary from one patient to the other. They can also appear as a single calcified mass or in clusters (multiple salivary stones are identified in 25% of the patients diagnosed with this condition). In the majority of the situations, the salivary stones appear at the level of the submandibular glands, these being located at the back of the mouth, on both sides of the jaw. The calculi can also appear at the level of the parotid glands, these being located in front of the ears, on both sides of the face. In regard to the size, it is known that the calculi affecting the submandibular glands are larger than the ones appearing in the parotid glands.
Symptoms of Sialolithiasis
First and foremost, it should be mentioned that the symptoms of sialolithiasis depend on whether the obstruction caused by the salivary stones is complete or partial. The size of the calculi is also important, as it can cause more or less pressure on the respective salivary gland.
When the salivary glands have become infected due to the salivary stones, these are the symptoms that the patient is going to suffer from:
- Pain – this comes and goes, being aggravated around mealtimes, due to the stimulation of the salivary glands. If the pain subsides in a short period of time, this might mean that the obstruction is partial.
- Inflammation of the salivary glands – the swelling comes and goes as well, being aggravated around mealtimes and slowly subsiding afterwards (also suggestive of a partial obstruction).
- The salivary glands become tender.
- If the calculi are located at a close distance from the salivary ducts, these can be palpated (felt as a hard lump). In some situations, the patient can feel this lump right under the tongue (suggestive that the salivary stone is near the submandibular duct orifice).
- If the obstruction is complete, no saliva is released from the duct.
- In the situation that there is an infection, the floor of the mouth presents a distinct, red color; pus can also be discharged from the respective duct.
- The lymph nodes in the cervical area can be swollen due to infection.
- Dry mouth (due to the reduced flow of saliva)
- Difficulty swallowing (dysphagia) or opening the mouth
- Systemic symptoms (suggestive of a bacterial infection)
- Fever
- Nausea, vomiting
- These symptoms are accompanied by local changes, such as foul taste in the mouth and redness in the affected area
It should be noted that, in case of chronic obstruction, the respective salivary gland can become atrophied. In such situations, the patient will not present any symptoms – the condition becomes obvious only in the situation of a secondary infection.
Causes
These are the most causes that lead to the appearance of sialolithiasis:
- Abnormality in the metabolism of the calcium
- Dehydration
- Reduction in the regular flow rate of the saliva
- Modified pH of the saliva (due to infection in the oropharyngeal area)
- Precipitation of mineral salts (due to the altered solubility of crystalloids)
- Accumulation of food debris, bacteria and foreign bodies at the level of the salivary gland ducts
- The sphincter mechanism of the salivary duct presents abnormalities, these contributing to the formation of salivary stones
- Salivary disease – chronic sialadenitis
- Gout – main composition from uric acid crystals
- Medication – taking certain medication, such as drugs to keep the blood pressure under control or allergy medication (antihistamines), can reduce the production of saliva at the level of the salivary glands (thus favoring the formation of calculi)
- Reduced food intake – you might not be aware of this fact but not eating enough food contributes to the reduction of saliva production (same as above, such actions favor the formation of salivary stones)
- Trauma and local inflammation due to different injuries
- Chronic conditions – saliva stasis (with associated changes in the composition of the saliva)
- Infection
- With viruses – mumps
- Bacterial – most commonly with: staphylococcus aureus, streptococcus viridans, streptococcus pneumonia, haemophilus influenza
Pictures of Sialolithiasis
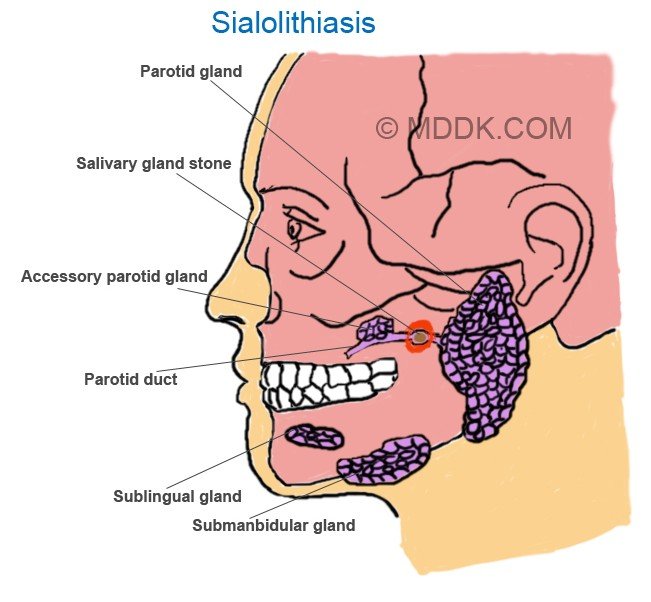
Sialolithiasis Picture 1 – Diagram showing Salivary gland stond along with various other parts including Parotid gland, Accessory parotid gland, Parotid duct, Sublingual gland, Submanbidular gland.
Diagnosis
These are the main methods used for the diagnosis of sialolithiasis:
- Patient medical history
- Recurrence of salivary stones and/or infections
- Onset and duration of symptoms
- Recent operative history
- Recent dental work
- Thorough medication history
- Immunization history – measles, mumps, rubella
- History of autoimmune conditions
- Surgical intervention history
- History of radiation therapy
- Recent health changes – weight loss, identification of a mass, swollen lymph nodes
- Physical examination
- Visual scanning – identification of inflammation and redness in the following areas: submandibular, preauricular and postauricular
- Intraoral examination – analysis of the salivary ductal orifice (in case of salivary stones, this is inflamed and red in color)
- Massage of the salivary gland – allows for the inspection of the saliva; in case of infection, a white secretion will appear through the salivary duct (purulence can be only identified through the examination of the ductal opening)
- Manual palpation of the parotid gland – check the consistency of the gland (recommended – bimanual palpation)
- Palpation extended to the floor of the mouth; the soft tissues of the tongue, cheek and neck should be examined as well
- The examination should be made for all the salivary glands – identification of existent masses, analysis of symmetry, examination for any discharge.
- Blood testing
- While blood cell count – increased levels suggestive of infection
- C-Reactive protein increased – sign of infection
- Serum amylase increased – another sign of infection
- X-ray – used for the confirmation of the diagnosis (the salivary stones are visible on the X-ray films)
- Sialography – radiographic examination of the salivary glands (contrast substance injected into the salivary ducts); the result of the investigation is known as sialogram. It is important to mention that, if an active infection is suspected, this investigation is not recommended (the infection can become exacerbated). This investigation allows for the visualization of the ductal system, thus making it easier for the doctor to identify any strictures or dilatations. Filling defects can also be identified with the help of sialography.
- Ultrasound – used for the confirmation of the diagnosis as well, recommended after the clinical examination of the patient. The advantage of the ultrasound is that it allows not only for the visualization of the salivary stones but also of the gland itself. If the obstruction is acute, the gland is going to appear enlarged and the salivary ducts dilated. The advantages of the ultrasound investigation relate to it being a non-invasive and non-painful measure. However, the ultrasound has a limited value when it comes to calculi that are located in the deep portion of the submandibular gland.
- Computer tomography (CT) – useful investigation, allows for the salivary stones at the level of the glands and the ducts to be visualized. The CT can also be used for the evaluation of the respective salivary gland. Through the CT, one can determine whether the salivary gland is atrophied or not (sign of chronic obstruction). The smaller calculi might not be visible on the CT. However, this investigation is highly useful when it comes to the identification of calcifications, intraparenchymal stones included.
- MRI – perfect investigation for the assessment of the salivary stones. Also recommended in order to make the difference between the acute and chronic obstruction of the salivary gland. If the obstruction is acute, the salivary gland appears enlarged and inflammation is present in the area. On the other hand, if the obstruction is chronic, the salivary gland presents a smaller size and signs of atrophy might already be present.
The radiographic investigation of the salivary stones is extremely useful in confirming the diagnosis. As it was already mentioned above, the salivary stones are visible on the radiographic films. However, it is important to keep in mind that not all the calculi are radiopaque. With the help of the X-rays, one can visualize submandibular stones (80-90%) and parotid duct stones (60%).
The differential diagnosis can be made with the following medical conditions:
- Hemangioma
- Phlebolith
- Atherosclerotic calcification
- Lymphadenitis
- Dental abscess
It is important to understand that film defects might influence the results of investigations, such as the sialography. In general, these film defects are due to injecting a bubble of air along with the contrast substance. They can also appear due to a tumor or a blood clot being present in the respective area. Repeating the said investigation is always a good idea, so as to confirm the correct diagnosis.
Treatment
In general, the treatment for sialolithiasis refers to non-invasive measures. Depending on the size of the calculi, the doctor might recommend an increased intake of fluids, moist heat therapy and anti-inflammatory medication. Bitter or sour foods and beverages are recommended, as they can stimulate the flow of saliva and dislodge the salivary stones. For example, the doctor might encourage the patient to consume a piece of citrus fruit – the increased salivation will cause the salivary stones to become dislodged on their own.
A special massage can also be applied, in order to stimulate the dislodging of the salivary stones. Shock wave therapy has also been found to be highly effective in the treatment of sialolithiasis. This procedure is also known as extracorporeal shock wave lithotripsy, with the shock waves being actually used in order to break the salivary stones into smaller pieces. The procedure can be done with local or general anesthesia. More recently, symptomatic salivary stones have been removed through a procedure known as endoluminal balloon dilatation, followed by the extraction of the respective calculi.
In some situations, the doctor might recommend a minimally-invasive procedure, meaning sialendoscopy. For this procedure, the doctor will place a camera through the salivary duct and remove the calculi using specific techniques. In more serious cases, surgical intervention is recommended. The removal of the salivary stones is performed by the ENT or oral surgeon, the procedure being known as sialectomy. If the patient suffers from recurrent salivary stones, the surgeon will decide to remove the salivary duct completely. Antibiotics are administered, in order to prevent the infections that may be caused by the obstructing salivary stones. Among the recommended oral antibiotics, there are: Augmentin, Cefzil, Ceftin and Clindamycin. During the period of the treatment, it is recommended to avoid caffeine and alcohol – these have diuretic properties and they can add to the already existent dehydration.
Prognosis
In the majority of the patients, the prognosis is positive, as the salivary stones are removed without any complications. If the patient suffers from recurrent salivary stones or infections at the level of the salivary glands, the surgical removal might be essential. The surgical removal of the gland presents a series of risks, including related to nerve injury. The doctor will take you through the risks associated with each procedure, making sure that you are comfortable with it.
Prevention
Poor oral hygiene is considered a risk factor for the appearance of salivary stones, so maintaining an excellent oral hygiene is a good preventative measure. However, some of these calculi are the result of an infection and this cannot be prevented.
