Dislocated Shoulder
What is a dislocated shoulder?
Anatomically speaking, the shoulder joint is the most mobile joint in the body, having the possibility to move the arm in many directions. This ability comes from the fact that the shoulder joint is one of the most complex joints in the human body but it also increases the risk for dislocation to occur. This is in fact the most dislocated joint in the body.
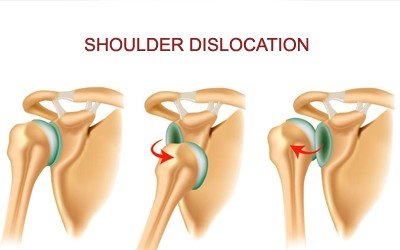
The dislocation occurs when the head of humerus leaves its normal socket through a forced mechanism. The dislocation of the humerus from the glenoid fossa can happen in more than just one direction and the location of the humeral head will also give the description of the dislocation. There are many different types of dislocations but two of the most common ones are the anterior and posterior dislocation. In the anterior dislocation, the humeral head has reached a position in front of the joint (this type of dislocation accounts for 90% of all cases of dislocated shoulder). The posterior dislocation is the one in which the humeral head has reached the shoulder blade. Rare cases included inferior and intrathoracic dislocations.
Symptoms

Dislocated Shoulder Pictures
These are the most common symptoms of a dislocated shoulder:
- Excruciating pain – the pain will be so intense that the patient will refuse arm movements of any kind.
- Spasms of the muscles surrounding the shoulder joint.
- Inflammation or bruising around the shoulder joint.
- Numbness or tingling.
- Tenderness of the shoulder and sometimes the collarbone.
- No palpable bone on the side of the shoulder.
- In case of anterior dislocation:
- Specific position of the arm (a little bit away from the body)
- Pain is relieved by supporting the affected arm with the other hand
- Damage to the axillary artery and nerve – paralyzed deltoid muscle and unilateral deltoid muscle atrophy
- Additional damage to the suprascapular nerve and radial nerve
- Shoulder has a specific appearance (as the humeral head is no longer in its socket, the shoulder might appear in a lower level, compared to the healthy one)
- Upon physical examination, a bulge can be palpated in front of the shoulder joint
- Pain can lead to the following systemic symptoms:
- Nausea
- Vomiting
- Excessive sweating
- Weakness
- Fainting.
Causes of a dislocated shoulder
These are the most common causes that lead to the appearance of a dislocated shoulder:
- In young people:
- Trauma
- Sports
- Falls
- In older people – the dislocation appears out of a combination of weakened joints and muscles plus a blunt force applied to the shoulder joint.
- Anterior dislocations occur most often when the shoulder is in a vulnerable position, such as the one in which the arm is held over the head, the elbow is bent and an outside force is applied to the shoulder joint.
- Posterior dislocations are rare but when they do occur, they have three main causes:
- Lightning strike
- Electrical injury
- Seizure
- Sports injuries lead often times to dislocated shoulders:
- Contact sports – football, hockey (the shoulder is a vulnerable position when throwing the ball)
- Sports with an increased risk for falling – skiing, gymnastics, volleyball (the shoulder is in a vulnerable position when hitting the ball)
- Different traumas to the shoulder can lead to dislocation:
- Motor vehicle accident – hard blow to the shoulder (strong force impact)
- Falls can lead to shoulder dislocation as well:
- Falling on an outstretched hand
- Falling from a ladder
- Tripping on different things (house accidents).
Diagnosis
These are the most common methods used for the diagnosis of the dislocated shoulder:
- The diagnosis should be confirmed as soon as it is possible, as there are concerns related to the extreme pain and the joint relocation has to performed in the most efficient manner.
- The doctor will talk to the patient about the way the injury to the shoulder has occurred and the circumstances surrounding it.
- It will be important to mention to the doctor whether you have suffered previously from dislocated shoulder joints or not.
- Be sure to mention if you suffer from any allergies, as a topical anesthetic will be used for the shoulder dislocation reduction.
- The physical examination is the most important element of diagnosis, as it will concentrate to determine whether the shoulder appearance is normal and rounded or the shoulder appears to be squared off. Often times, the loss of the normal rounded appearance is identified (deltoid muscle is affected) and the humeral head can be palpated in front of the joint.
- The inability to move the arm in any direction is also a sign necessary for the confirmation of this diagnosis.
- The doctor will also try to identify if the blood and nerve supply in the arm have been affected:
- Pulse in wrist and elbow
- Test for sensation
- X-rays in anterior and lateral plans will be performed not only for the confirmation of the diagnosis but also to ensure that there are no additional bone fractures that need to be treated as well.
Treatment
The main scope of the treatment is to reduce the dislocation, that is to bring the humeral head back into its anatomical socket. The closed reduction performed with local anesthesia is often successful but there are situations when the open reduction (surgical intervention) is more recommended.
These are the most common methods used for the closed shoulder reduction:
- Scapular manipulation – the shoulder blade is rotated, the humeral head is dislodged and then the relocation occurs spontaneously.
- External rotation (Hennepin maneuver) – the elbow is flexed to 90 degrees and the shoulder gradually rotated outward. The doctor continues to push the arm gently, until the shoulder relocation occurs.
- Milch technique – this is a similar method to the one presented above, the difference lying in the fact that the arm is lifted above the head in order for the shoulder relocation to occur.
- Traction-counter traction – in this method, the first step is to loop a sheet around the armpit. Then, one person will pull down on the arm and another person will pull on the sheet, basically applying counter traction, until the shoulder relocation occurs.
Dislocated shoulder surgery
The open reduction is recommended in the case where a tendon, ligament or piece of broken bone blocks the shoulder joint and prevents the humeral head from returning to its anatomical socket. Also, the dislocated shoulder surgery is recommended in patients who cannot change their occupation (this presenting an increased risk for shoulder dislocation) and also in the case of recurrent shoulder dislocation or the constant practicing of high risk sports. The arthroscopic approach has provided the best results for the open reduction of dislocated shoulders.
Recovery time
The recovery time depends on the severity of the shoulder dislocation and whether nerve or artery damaged have occurred. After the closed reduction, the doctor will put the shoulder in a sling or shoulder immobilizer, so as to guarantee that the shoulder joint stays immobilized and that the area heals properly. Anti-inflammatory medication will be recommended during the recovery period and sometimes the doctor will even recommend narcotic medication for severe pain. Ice packs can be applied to the affected area in order to reduce the pain or inflammation.
The recovery period can be of several months, during which you will have to follow the instructions of the doctor and go to physical therapy after the immobilizer has been removed. You need to rest your shoulder and avoid high risk activities, especially those that present a potential for a new dislocation. Do not be afraid however to move the joint otherwise the whole area will become stiff and you will lose the normal range of motion or suffer from muscle atrophy.
Physical therapy is essential in order to reduce the recovery time and guarantee a better healing of the area. A good physical therapy program can help you regain the normal range of motion in the shoulder and it will also prevent abnormal adherence from forming. Moreover, the exercises will be more and more difficult, so as to allow not only for an improvement in the range of motion but also to guarantee that all of the muscles in the shoulder joint are strengthened.
Pictures